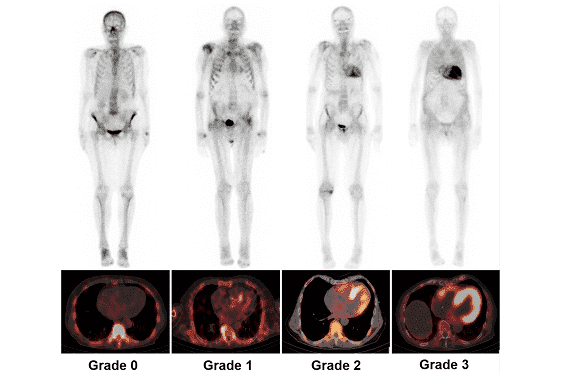
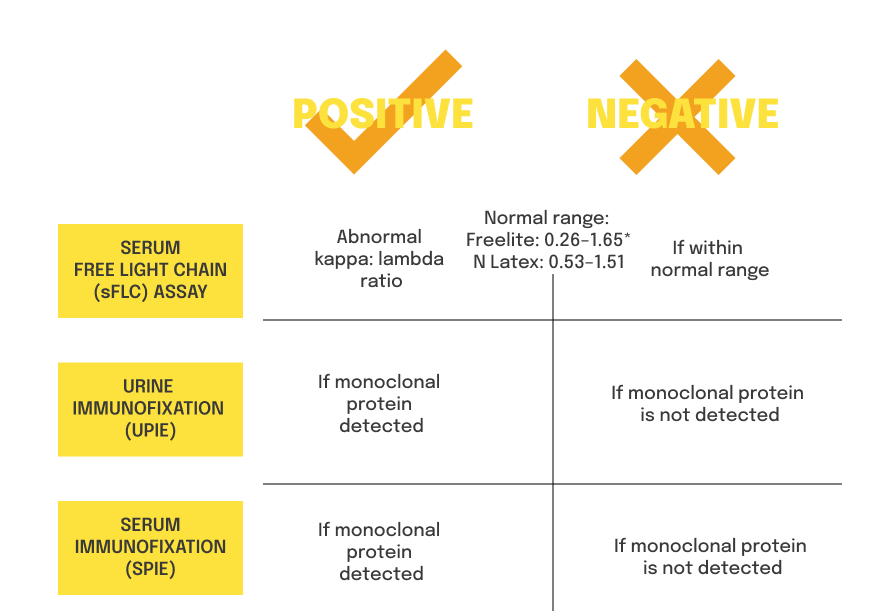
In this video, Dr Garcia-Pavia discusses the role of scintigraphy in diagnosing ATTR-CM, as well as how to interpret other diagnostic screening tests for ATTR-CM.
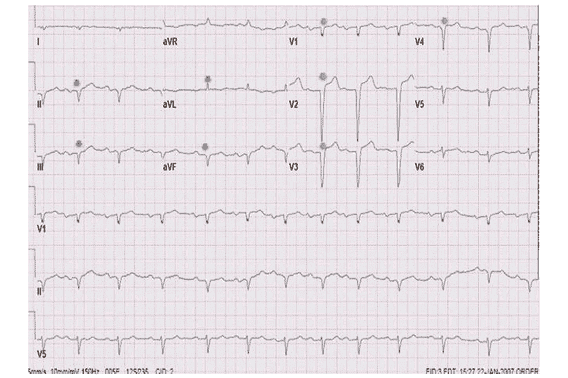
ECG4
- Pseudo-infarction pattern
- QRS voltages disproportionate to LV wall thickness
- Atrioventricular block in the presence of LVH
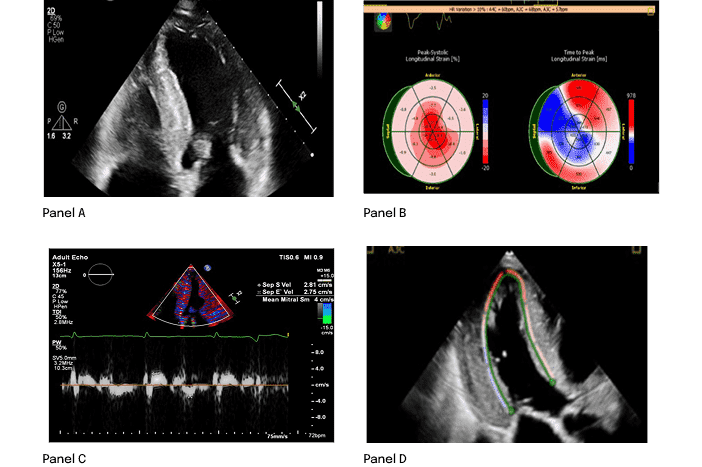
ECHO4
- Hypertrophic phenotype with infiltrative features
- Restrictive LV filling with RV wall thickening
- Low septal and lateral e′
- Reduction in global longitudinal strain
Proactively looking for these findings in regular clinical practice may facilitate an ATTR-CM diagnosis5
Once ATTR-CM is suspected, ACT FAST. Learn about the diagnostic process to confirm ATTR-CM

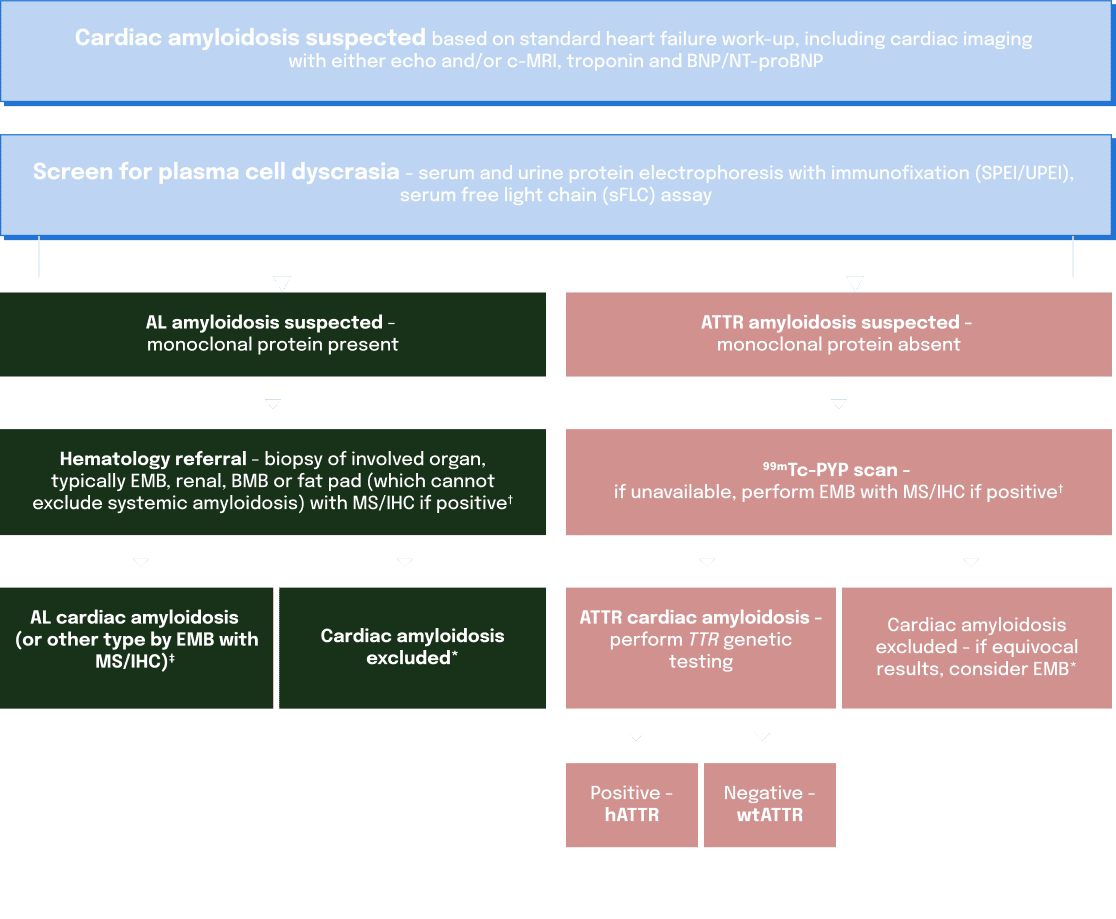
* Endomyocardial biopsy should be performed if non-invasive evaluation is equivocal or negative despite a high index of clinical suspicion.7
† Tissue biopsy analysis includes Congo red staining for amyloid deposits.7
‡ A diagnosis of AL cardiac amyloidosis should prompt urgent hematology referral.7
hATTR and wtATTR can present differently, and may require a
different treatment and management strategy1,6
Detection of a pathogenic TTR variant allows for
testing of family members
and earlier detection of symptoms and treatment intervention8,9
TREAT
Specific ATTR-CM treatments are available.10 Initiating these treatments as early as possible can lead to improved outcomes10
OR REFER
ATTR-CM is a rapidly progressive disease.4 It is vital to ACT FAST. Referral to a specialist centre may ensure patients get the right treatment, sooner
Once ATTR-CM is confirmed, ACT FAST. Learn about how patients may present in your practice